Supporting Births at Texas Children’s Pavilion for Women: What You Need to Know Before You Choose This Hospital
I’ve supported seven births at Texas Children’s Pavilion for Women in the Texas Medical Center in 2025. All seven were inductions. All seven required significant advocacy. And all seven taught me something important about what families need to know when choosing this hospital.
As both a labor and delivery nurse who has worked contracts at Texas Children’s and a certified doula through The Birthing Noire Collective, I can give you the insider perspective that most people don’t get until they’re already admitted and laboring.
Texas Children’s has a world-class reputation. The NICU is internationally recognized. The Fetal Center is among the best in the nation. The building is beautiful, the views are stunning, and the technology is cutting-edge.
But there’s a gap between the hospital’s reputation and what actually happens on the labor and delivery floor—especially in the past year.
If you’re considering Texas Children’s for your birth, here’s what you need to know.
Why Families Choose Texas Children’s
Let me start here, because this matters: Texas Children’s is exactly where you want to be if your baby has a known medical issue that will require immediate NICU care.
The NICU team at Texas Children’s is exceptional. They communicate clearly with families, explain what’s happening with baby, and provide world-class neonatal care. If you know prenatally that your baby will need specialized medical support at birth, Texas Children’s Pavilion for Women gives you direct access to that expertise.
The Fetal Center is also unmatched. If you’re working with maternal-fetal medicine specialists for high-risk pregnancy complications, congenital issues, or complex medical situations, you’re in expert hands.
This is what Texas Children’s does best: high-risk, medically complex pregnancies and births.
What’s Changed at Texas Children’s
Here’s what I need to be honest about: Texas Children’s Pavilion for Women is not the same hospital it was two years ago.
In summer 2024, Texas Children’s laid off their entire midwifery program—six full-time certified nurse midwives and one part-time CNM. The hospital cited financial challenges including lost Medicaid revenue and rising expenses.
Around the same time, nursing staff were also laid off.
Since then, the culture on the labor and delivery floor has shifted. The care is still medically excellent, but the atmosphere feels different. Staff seem less engaged, less enthusiastic. Burnout is palpable.
I say this not to criticize individual nurses or providers—many of whom are working incredibly hard under difficult circumstances—but because families deserve to know what environment they’re walking into.
Understanding the Teaching Hospital Model
Texas Children’s Pavilion for Women is a teaching hospital. This means residents are heavily involved in your care.
Most families know ahead of time that there will be residents on the unit. What surprises them is how little they actually see their own OB physician and how much they communicate with their doctor through residents instead.
Here’s the typical structure:
- Residents manage the majority of your labor
- Attending physicians (your OB) come in for emergencies, do rounds, or appear when delivery is imminent
- Some providers hand over care to the hospitalist on call after certain hours (you need to clarify this with your OB prenatally)
This isn’t necessarily bad—residents are doctors completing specialized training. But it does mean:
- You may not see your actual OB until you’re pushing
- Decisions about your care are filtered through residents first
- Your birth plan gets interpreted by multiple people with varying levels of experience

The Resident Factor: What It Means for Your Birth
Residents at Texas Children’s tend to be intervention-oriented. This is common in teaching hospitals where residents are learning to manage complications, but it impacts how your labor is approached.
Common interventions residents push for:
- Pitocin as the primary induction method (even when Bishop score suggests Cytotec would be more appropriate)
- Cook balloon for cervical ripening (often combined with Cytotec)
- Epidurals (sometimes before you’ve even asked)
- Artificial rupture of membranes (breaking your water)
- Delivery in lithotomy position only (flat on back, feet in stirrups)
The pushback to these recommendations typically comes in the form of “patient education”—which sounds good but often means biased information that emphasizes why the intervention is necessary without fully explaining alternatives or giving you true informed consent.

Real Examples from My Texas Children’s Births
Example 1: Pushing position limitations
I had a client who wanted to push on her hands and knees. She kept telling the resident she wanted to push in that position. The resident kept asking her to lay on her back. Mom said no and stayed on hands and knees.
When baby was crowning, the nurse caught the baby because the resident was too focused on trying to get mom onto her back in the resident’s preferred position rather than supporting the birth that was actually happening.
Residents are generally not comfortable delivering in any position other than lithotomy (flat on back). This limits your options during pushing, even when alternative positions might help baby descend or reduce tearing.
Example 2: Inappropriate induction method
I supported a client who was being induced. She had a thick cervix and, according to her Bishop score, would actually benefit from Cytotec for cervical ripening before Pitocin.
The resident wanted to use Pitocin immediately and spent significant time “educating” mom on why Pitocin was the right choice—instead of honoring her wish to speak with her OB about using Cytotec first.
The nurse stepped in and helped us advocate. This is important to note: sometimes the nurses at Texas Children’s are your allies in pushing back against resident preferences that don’t align with evidence or your body’s needs.
Example 3: Jumping to cesarean with an OB
One of my clients was pushing with little to no progress. Baby’s heart rate showed stress. The attending OB (not a resident) suggested cesarean—but without trying:
- Position changes
- Turning off the Pitocin to let baby and mom recover
- Laboring down to let mom rest
- Pushing with every other contraction instead of every one
Using my knowledge of reading fetal monitoring strips, I could see that baby had good reserve (moderate variability) despite some concerning decelerations. I advocated for these alternatives first. Mom was able to deliver vaginally with a healthy baby and great Apgar scores.
This is what advocating at Texas Children’s looks like: you have to know when to push back, how to push back, and what alternatives to request—whether you’re dealing with residents or attending physicians.
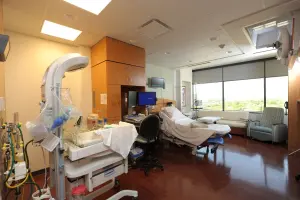
What the Facilities Are Like
Despite the cultural challenges, the physical environment at Texas Children’s is excellent.
The labor rooms are:
- Spacious and comfortable
- Beautifully appointed with large windows and great views
- Equipped with tubs for hydrotherapy
- Well-stocked with dad couches and recliners
- Large enough for movement and position changes
They have comfort carts with:
- Diffusers for aromatherapy
- Labor combs
- LED candles
- Other comfort items for client use
Wireless monitoring (Novii system) is available but:
- There’s a criteria checklist to be eligible
- It’s hit-or-miss with WiFi connectivity (not uncommon at any Houston hospital)
- They also have portable wired monitors as backup

Admission and Triage
First-floor triage: Only mom is allowed in. Dad and doula wait in the waiting area just outside the doors.
Larger triage area: There’s also a bigger triage space where dad can be with mom (I’m not certain this is specifically on the second floor, but there is a larger triage option where partners are allowed).
Access: Your doula will need an access code to visit on the labor and delivery unit. The code doesn’t change, but your nurse will need to provide it so your doula can access the unit.
The Nursing Staff: Hit or Miss
Here’s where I have to be completely honest: the nursing staff at Texas Children’s is inconsistent.
Some nurses are wonderful—friendly, skilled, caring, attentive to patient autonomy, excellent bedside manner. They make a difficult environment feel manageable. Sometimes these nurses become your advocates when residents push interventions that don’t align with evidence or your preferences.
Other nurses seem overworked, burned out, and frankly mean. Their presence can negatively affect mom’s mood and birth experience in ways that are hard to recover from.
For unmedicated births: Nurses will help with positioning and comfort measures, but if a doula is present, they generally give the doula space to work and step back.
For epidural births: Nurses are very skilled at positioning patients who have epidurals and regularly help with peanut ball positioning and side-lying techniques.
The reality: You don’t get to choose your nurse. If you’re not happy with your assigned nurse, you can request a different nurse. Most families don’t know this, but it’s your right and sometimes necessary at Texas Children’s.
Birth Plans and Interventions
Staff at Texas Children’s do read birth plans. The challenge is that with residents managing your care, birth plans take lots of active advocating to stick to.
Residents often have their own agenda when they walk into your room. They’ve reviewed your chart, they have a plan in mind (often based on what they’re comfortable with rather than what’s best for your specific situation), and your birth preferences may not align with what they were taught is “best practice.”
Once you’re firm with your “no,” they typically respect it—but expect pushback first.
This means:
- You’ll hear why the intervention is necessary
- You’ll get education (often biased toward intervention)
- You’ll need to hold your boundary and ask for alternatives
- Eventually, they’ll respect your decision
The good news: If you’re prepared for this dynamic and know how to advocate, you can have a positive birth experience at Texas Children’s. All seven of my clients in 2025 ultimately felt respected, but we had to work for it.

Epidurals and Pain Management
Every mom is consented for epidural upon admission to labor and delivery—whether she wants one or not.
The rationale: it saves time if mom decides she wants an epidural later. All the paperwork is already done, anesthesia can come quickly.
For moms planning unmedicated birth, this can feel pushy and insensitive, especially when your birth plan explicitly asks not to be offered pain medication.
Anesthesia response time is generally fast, though if there’s an emergency elsewhere, you’ll wait (this is true at any hospital).
Induction at Texas Children’s: What to Expect
All seven of my 2025 clients at Texas Children’s were induced. The most common reasons:
- Low amniotic fluid
- Post-dates (going past 40-41 weeks)
Induction scheduling challenges: Texas Children’s is a very busy facility. Inductions frequently get pushed back multiple times due to high patient volume. Families wait hours for a bed. Some are called in the middle of the night (2 am, 3 am) to start their induction.
This is brutal for moms because it:
- Disrupts sleep and rest right when you need it most for labor
- Affects your nervous system’s ability to cope with contractions
- Starts you off exhausted before labor even begins
Induction methods: They discuss all options, but residents often advocate hard for their preferred methods regardless of your Bishop score or personal preference. I’ve seen residents push for Pitocin when Cytotec would be more appropriate based on cervical readiness. This is doctor preference being pushed as “best practice.”
Despite all this, unmedicated birth after induction is possible at Texas Children’s. I’ve supported clients who achieved it. But it requires strong advocacy, continuous support, and nurses who are willing to work with you.
Cesarean Policies
Doulas are not allowed in the OR at Texas Children’s. Only one support person (typically your partner) can accompany you during cesarean birth.
As your doula, I support you up until you go into the OR and am there waiting when you come out.
Postpartum Care
Golden hour: Texas Children’s does respect the golden hour and supports immediate skin-to-skin when mom and baby are both stable.
Dedicated bay nurse: After delivery, there’s a separate nurse for mom and a separate nurse for baby. I find this very helpful—one person is focused on your recovery while another tends to your newborn.
Mother-baby care: Mom and baby are kept together in the same room.
Lactation support: Available and generally helpful.
Logistics
Parking: Easy. Valet available or you can park in the garage.
Navigation: Straightforward to find labor and delivery.
Doula rest space: Waiting area on the unit or the cafeteria. The cafeteria space is quiet and comfortable during long labors.
The NICU: Where Texas Children’s Shines
If your baby needs NICU care, this is where Texas Children’s excels.
The NICU team is exceptional at:
- Communicating with families clearly and compassionately
- Explaining what’s happening with baby’s condition and care plan
- Providing world-class neonatal intensive care
- Supporting families emotionally through scary situations
If you know prenatally that your baby will need NICU support, this is where you want to be.
My Honest Assessment as Both Doula and L&D Nurse
Supporting births at Texas Children’s has become harder.
The building is beautiful. The technology is excellent. The NICU is world-class. But the culture on the labor and delivery floor has shifted in ways that make advocacy more necessary and more difficult.
Staff aren’t showing up to work with the same enthusiasm and engagement they once had. Burnout is affecting how families are treated. Residents are intervention-heavy without always providing truly informed consent. Even attending physicians sometimes jump to cesarean without exploring alternatives first.
That said, I still recommend Texas Children’s Pavilion for Women in specific situations:
Choose Texas Children’s if:
- Your baby has a known medical issue requiring immediate NICU care
- You’re high-risk and need Level IV maternal care
- You’re working with the Fetal Center for complex fetal conditions
- You have access to specific providers you trust there
- You’re prepared to advocate firmly for your birth preferences

How to Prepare for Birth at Texas Children’s
If you’ve decided Texas Children’s is right for you—either because of medical necessity or personal choice—here’s how to set yourself up for success:
1. Clarify your provider’s availability. Ask your OB: “Will you be the one delivering me, or will you hand over care to a hospitalist after certain hours? At what point do residents hand over to you?”
2. Create a clear, firm birth plan. Include:
- Your priorities and “why”
- Specific interventions you want discussed before implementing
- Your preferred pushing positions (and that you do NOT consent to being forced into lithotomy)
- Your approach to pain management
- Requests for alternatives before jumping to cesarean
3. Prepare to advocate—or hire someone who will. This is not the hospital where you can just show up and trust everything will align with your preferences. You need either:
- Strong self-advocacy skills
- A partner who’s prepared to speak up firmly
- A doula who knows how to navigate residents and teaching hospital culture
4. Know you can request a different nurse. If your nurse’s attitude is negatively affecting your experience, you can ask for a different nurse. You don’t have to suffer through bad bedside manner.
5. Understand the resident dynamic. Expect intervention discussions. Prepare responses. Know when to hold firm and when to genuinely consider recommendations. Remember that residents are often pushing their comfort zone preferences (like Pitocin over Cytotec, or lithotomy position over hands-and-knees) rather than what’s actually best for your body.
6. If your induction gets pushed back, advocate for better timing. If they’re calling you in at 2 am, ask if you can come in the morning instead. Starting exhausted makes everything harder.
7. Specifically address pushing positions in your birth plan. State clearly that you want the freedom to push in whatever position feels right to your body. Make it explicit that you do not consent to being coached into lithotomy position if that’s not what you want.

Why Doula Support Matters Even More at Texas Children’s
At hospitals where staff are collaborative and birth plans are enthusiastically supported, doula support is helpful but not essential for everyone.
At Texas Children’s, doula support is critical if you want to maintain your voice and your preferences.
Here’s why:
- Residents rotate frequently – you’ll have multiple people managing your care who don’t know you
- Intervention pressure is constant – someone needs to help you evaluate recommendations objectively
- Staff are inconsistent – continuous support from someone who’s there for YOU makes up for nursing gaps
- Teaching hospital dynamics are complex – navigating who has authority and when requires insider knowledge
- My L&D nursing background matters here – I can read fetal monitoring, understand when interventions are genuinely necessary, and know when there are alternatives to try first
- Residents have preferences that don’t always align with evidence – I can help you push back when a resident wants Pitocin but your cervix needs Cytotec, or when they want you flat on your back but hands-and-knees would help baby descend
That advocacy I provided when the OB wanted to jump to cesarean without trying position changes first? When I helped the client whose resident was pushing Pitocin inappropriately? When the nurse and I worked together to support the mom who wanted to push on hands and knees? That’s what doula support looks like at Texas Children’s.
Planning to birth at Texas Children’s and want support from someone who knows how to navigate this specific hospital culture?
Book your free Consultation to discuss how The Birthing Noire Collective can help you advocate effectively at Texas Children’s Pavilion for Women. Because at this hospital, having insider knowledge and advocacy skills isn’t optional—it’s essential.
Frequently Asked Questions
Q: Can I have a doula at Texas Children’s Pavilion for Women?
A: Yes, doulas are allowed on the labor and delivery unit. Your doula will need an access code from your nurse to get onto the unit. However, doulas cannot attend cesarean births in the OR—only one support person is allowed. I’ve found that nurses are generally more welcoming to doulas than the residents/physicians are.
Q: Will I see my own OB during labor?
A: Probably not much. Residents manage the majority of labor, and attending physicians typically come in for emergencies, during rounds, or when delivery is close. Some providers also hand over care to the hospitalist on call after certain hours—clarify this with your OB prenatally.
Q: What if the resident recommends an intervention I don’t want?
A: You can decline. Expect them to provide education about why they believe it’s necessary. Ask for alternatives. Be firm if you’re comfortable with your decision. Once you’re clear about your “no,” they typically respect it, though there may be initial pushback.
Q: Can I push in positions other than flat on my back?
A: Yes, but you’ll likely need to advocate for it. Residents at Texas Children’s are generally most comfortable with lithotomy position (flat on back, feet in stirrups) and may push you to deliver in that position even if another position would be better for you. Put your preferred pushing positions explicitly in your birth plan.
Q: Can I have an unmedicated birth at Texas Children’s?
A: Yes, though it requires strong advocacy. I’ve supported clients who achieved unmedicated birth there, including after induction. Nurses will help with positioning if you ask, but expect repeated epidural discussions including being consented for epidural upon admission even if you don’t want one.
Q: What if my induction gets delayed?
A: This happens frequently at Texas Children’s due to high patient volume. You may wait hours for a bed or get called in the middle of the night. Ask if alternative timing is possible—starting exhausted makes labor much harder.
Q: Is Texas Children’s a good choice for low-risk, straightforward pregnancies?
A: Honestly, probably not. Texas Children’s excels at high-risk, medically complex pregnancies. If you’re low-risk, there are other Houston hospitals with more collaborative cultures and less intervention-heavy approaches that might be better fits.
Q: What happened to the midwives at Texas Children’s?
A: Texas Children’s laid off their entire midwifery program in summer 2024 (6 full-time and 1 part-time CNM). The hospital cited financial challenges. Midwifery care is no longer available there.
Q: Can I request a different nurse if I’m not happy with mine?
A: Yes! Most families don’t know this, but you absolutely can request a different nurse if your current nurse’s attitude or care is negatively affecting your experience.
Q: When is Texas Children’s the right choice?
A: Choose Texas Children’s if your baby has a known medical issue requiring NICU care at birth, if you’re high-risk and need Level IV maternal care, or if you’re working with the Fetal Center for complex fetal conditions. This is where their expertise truly shines.
I do earn a commission on the amazon products listed.



